To what extent did the World Health Organization’s delayed characterization of COVID-19 as a pandemic influence Canada’s failure to efficiently contain COVID-19?
Siya Duggal | Originally Published: 3 May 2026
Policy Brief: The GPHIN as Canadian Biological Surveillance’s ‘Crown Jewel’
A key lesson to take from the attached study is that Canada failed to respond effectively to COVID-19 due to domestic weaknesses, which were compounded by the World Health Organization (WHO) delaying its categorization of COVID-19. In 2025, WHO member states adopted the Pandemic Agreement, otherwise known as the “Pandemic Prevention, Preparedness, and Response Accord,” in an effort “to strengthen pandemic prevention, preparedness, and response.” However, since Canada’s failure to contain COVID-19 was not solely caused by international factors, Canada must address its domestic shortcomings to ensure it can safeguard Canadians against future disease outbreaks.
The key shortcomings in Canada’s COVID-19 response lie in the federal government’s inability to maximize intelligence from the Global Public Health Intelligence Network (GPHIN), identify the contagion’s transmission method, address weak points in the healthcare system, and successfully ensure federal-provincial collaboration. GPHIN is “the crown jewel in Canada’s biological surveillance apparatus” (Levy 2021, 3). Therefore, this policy brief suggests that in order to contain future contagions effectively, Canada should adopt a three-fold policy which maximizes the GPHIN, addresses known shortcomings in the healthcare system, and produces effective federal-provincial communication.
Maximize the Global Public Health Intelligence Network (GPHIN)
The Canadian government must address the structural problems identified by GPHIN’s 2021 independent review panel, which prevented intelligence from reaching decision makers (3). The government must also ensure GPHIN’s daily reports are formatted in a manner conducive to decision-making – i.e. that they are direct and concise – to avoid the inefficiency caused by the reports’ lengthy nature in COVID-19 (Fitzgibbon 2021, 4). Further, as explained by Margaret Bloodworth, leader of the independent review panel, to guarantee efficiency, the Canadian government cannot outsource GPHIN; it must remain under federal control (Levy and Wark 2021).
Finally, while GPHIN functions as an early-warning system for biological threats, Canada should also employ the tools it has access to via GPHIN to remain aware of global research on viruses. Despite Canada’s intelligence, it failed to recognize COVID-19 as airborne, while Japan and Finland did so early in the pandemic, with Finland publishing its findings in April 2020 (Read 2020; Craft 2020).
To improve GPHIN’s efficiency and ensure Canada’s public health guidance is accurate, the federal government should invest in expanding the 10-analyst team (Levy and Wark 2021).
Strengthen Federal-Provincial Relationships & Improve Healthcare
In COVID-19, GPHIN’s reports were sent to the Public Health Agency of Canada (PHAC) alongside provinces and territories, yet when March Break arrived, ineffective communication across Canada’s varying levels of government prevented the containment of COVID-19 (Vahed 2021). Thus, alongside maximizing the GPHIN’s capacity, Canada must also facilitate practical use of its findings by ensuring effective communication between GPHIN and provincial governments. In this vein:
- PHAC should invest in designated communication officers who would liaise between GPHIN and key decision-makers.
- Since education falls under provincial jurisdiction, the federal government must communicate with provincial governments to ensure Canada’s containment strategies account for travel that occurs during school breaks.
Moreover, since funding and national standards for healthcare fall under federal jurisdiction, the Canadian government should allocate funds and set standards which enable country-wide improvements in healthcare.
- That said, a limitation posed by Canada’s political structure would be that provincial governments have jurisdiction over how funds are allocated within their health system.
- Nonetheless, by ensuring effective communication of GPHIN information to provincial governments, the federal government can facilitate informed decisions.
On balance, Canada’s 4.5 million cases (as of July 2024) and 60,871 deaths (as of September 2024) reflected a catastrophic intelligence failure (“COVID-19 Epidemiology Update: Current Situation” 2024). Thereby, to ensure success in containing future contagions, Canada must take actions to maximize GPHIN’s position as the ‘crown jewel’ of Canadian health surveillance.
Introduction
SARS-CoV-2, i.e. COVID-19, is a pathogen that made history at the onset of the second decade of the 21st century. The World Health Organization (WHO) classified COVID-19 as a Public Health Emergency of International Concern (PHEIC) on January 30, 2020 and as a pandemic on March 11, 2020 (World Health Organization 2025). COVID-19 remained a PHEIC for over 3 years, with the WHO removing that status on March 5, 2023, given that COVID became a well-established ongoing disease (World Health Organization 2025). The removal of the PHEIC status does not mean the pandemic itself is over; in 2020 and 2021 alone, COVID-19 was directly or indirectly the cause of 14.9 million deaths worldwide (World Health Organization 2025; United Nations n.d.). COVID-19 remains an ongoing global health concern, with Canadians, as of December 2025, remaining at high risk of contracting the virus (“Canadian COVID-19 Hazard Index” 2025). It is also possible for future pandemics to ensue as new contagions arise. Thus, it is vital to examine and understand the reasons behind the global failure to contain COVID-19 before it transitioned into a pandemic.
COVID-19 transformed multiple aspects of life as societies became familiarized with concepts such as quarantine, work-from-home, and lockdowns. It was not the first time states responded to a contagion with a quarantine – quarantines have been implemented in response to diseases throughout history, be it in the Plague of Athens, Spanish Flu, or smallpox. COVID-19’s nature as a coronavirus was also not unprecedented. The world witnessed an epidemic caused by another coronavirus, SARS-CoV-1, in 2002-2003. That said, quarantine measures proved ineffective in combating COVID-19, and unlike the first coronavirus, SARS, COVID-19 became a pandemic. This discrepancy is perhaps explained by the increased interconnectedness of the world during COVID-19. Be it through digital connectedness via the internet or a physical increase in travel, the world during COVID-19 was not the same as it was during the SARS epidemic (“The Daily: Household Internet Use Survey” 2003; “Canada’s Internet Factbook 2019” 2019). COVID-19 also took place against a heightened access to scientific knowledge and resources in comparison to historical outbreaks such as the Spanish Flu and Plague of Athens. This increased scientific knowledge included response plans that had been developed in response to the 2002-2003 SARS epidemic (Levy 2021).
Given that countries had potential action plans and experience tackling a coronavirus in SARS, the question arises of whether a state that failed in addressing COVID-19 lacked the capacity to contain it or whether its response involved avoidable inefficiencies. To address this question, this study will explore the various facets underpinning a state’s pandemic response, including the role of the World Health Organization’s classification of the virus. This study focuses on: To what extent did the World Health Organization’s delayed characterization of COVID-19 as a pandemic influence Canada’s failure to efficiently contain COVID-19? In response to this research question, this paper argues that the World Health Organization’s delay in characterizing COVID-19 as a pandemic impacted Canada’s failure to efficiently contain the virus to some extent, but more significantly, Canada’s failure was a byproduct of domestic factors, such as failure to maximize its health intelligence, inaccurate public health guidelines, and lack of federal-provincial communication.
Literature Review
The efficacy of international organizations (IOs) is a notable area of debate in international relations. Some scholars suggest that IOs are merely instruments for the states that established them and therefore cannot independently affect state behaviour (Mearsheimer 1994, 7). Others suggest that while state influence remains, the autonomy and impact of IOs have largely increased (Reinelda and Verbeek 1998, 38-39). Recent studies present IOs as active participants who act as governors rather than bureaucracies, asserting that IOs derive autonomy and authority from expertise, conferred rational-legal authority, delegation, and moral claims (Barnnet and Finnemore 2004, 16). Nonetheless, IOs’ efficacy remains constrained by other factors such as access to resources (Cox and Jacobson 1973, 87; Gehring and Urbanski 2022, 1-25). Conflict also affects the operations of IOs, as when operating in war-torn areas, IOs face significant challenges, namely interference from non-democratic authorities (Zubytska 2024, 99). Further, IOs are scrutinized by various global actors, either for responding ineffectively or for focusing strongly on one concern while neglecting other issues (Zubytska 2024, 101). Particularly concerning the World Health Organization (WHO), scholars consider it the “central agency responsible for global surveillance of infectious disease” (Fitzgibbon 2021, 3). Scholars also reveal that the WHO was inefficient in responding to various outbreaks, including the 2014 Ebola outbreak, and this inefficiency is viewed as a byproduct of structural, cultural, political, and epidemiological factors (Kamradt-Scott 2018, 193-194; Wenham 2017, 1).
When examining the global spread of contagions, scholars have not only focused on the efficacy of IOs but also on the motivations of states in responding to contagions. Studies exploring SARS-CoV-1 highlighted that states underestimate viruses, and they hesitate to implement health policies which may negatively impact tourism and retail; for instance, Microbiologist Elizabeth Prescott revealed that Canadian officials ignored the WHO’s advisory that passengers departing from Toronto be screened by medical personnel (Price-Smith 2008, 147; Corby 2020). Research has also shown that states’ responses to pathogens are also influenced by the Liberal International Order’s sacrificial element, while scholars such as Andrew Price-Smith have noted that states’ responses to contagions are motivated by two central factors: fear and threats to their material interests (Barnett 2020, E128-30; Price-Smith 2008, 157). Price-Smith explains that after SARS-CoV-1, fear and threats to their material interests led states to invest in “global pathogen-surveillance systems and pathogen-containment regimes” (Price-Smith 2008, 157). Fear has also been posited as a key factor influencing states’ actions and thereby world politics beyond pathogens (Alfred 2019).
This paper contributes to the debate surrounding IOs’ efficacy by exploring the impact of the WHO’s delayed response on Canada’s efforts to address COVID-19. Rather than examining the inward causes of the WHO’s inefficiency, I focus on the outward impact, using Canada’s pandemic response as a case study to highlight the significant influence the WHO has over global health policy. In examining the domestic factors influencing Canada’s COVID-19 response, this paper also contributes to the discourse surrounding states’ response to contagions; it demonstrates how international and domestic factors work in tandem to shape a state’s response to contagions.
WHO’s Delayed Characterization of COVID-19 as a Pandemic
As argued by David Stasavage, suppression of information surrounding the virus by the Chinese state enabled the Wuhan outbreak (Stasavage 2020, E2). Even after hearing from its Wuhan office that a pneumonia-like virus had emerged on December 31, 2019, the WHO did not assemble its emergency committee until January 22, 2020 (Fitzgibbon 2021, 3). The assembly of this emergency committee is an obligation for the WHO under the 2005 International Health Regulations, i.e. IHR (Caffrey 2024).
Originally adopted in 1969 by the Health Assembly to prevent the spread of disease across borders, the IHR were updated in 2005 after the 2002-2003 SARS outbreak (Caffrey 2024). The 2005 IHR is a binding agreement between 196 countries, including all WHO member states, which aims to “prevent, protect against, control, and provide a public health response to the international spread of disease” (World Health Organization 2019; Rushton and Ferhani 2021, 3). A key step in achieving this goal is the calling of an IHR Emergency Committee, which advises the WHO Director-General on whether a given outbreak constitutes a Public Health Emergency of International Concern, i.e. a PHEIC (World Health Organization 2019). When the pneumonia-like virus emerged in Wuhan in December 2019, the WHO fulfilled its responsibility of calling for an emergency committee, but the one-month delay in doing so led to the organization failing to fulfill the IHR’s aim of preventing the international spread of diseases. By the time the WHO classified COVID-19 as a PHEIC on January 30 based on the emergency committee’s advice, the novel coronavirus had already spread outside China with cases documented in many countries, including Canada (“Public Health Agency of Canada’s COVID-19 Response: Lessons Learned” 2024; Fitzgibbon 2021, 3).
PHEIC is the strongest global alert that the WHO can formally make (Geddes 2023). This status triggers legally binding obligations which assist in coordinating an international response to the outbreak (Geddes 2023). That said, the most commonly used classification for COVID-19 is pandemic. While PHEIC is an official classification given to diseases by the WHO, pandemic is an epidemiological term which “describes the global spread of a pathogen” (Geddes 2023). The WHO defines a pandemic as when a new “virus emerges and spreads around the world, and most people do not have immunity” (“Health Topics: Pandemics” 2025). Despite pandemic not being a formal WHO classification, the WHO classified COVID-19 as a global pandemic on March 11, 2020, at which point global cases had surpassed 126,000. After this declaration, states took strong action against the pandemic; for instance, Canada decided to halt international flights. A question that arises here is that if the WHO is not responsible for declaring the start or end of a pandemic and it is not a legally binding designation, why do states’ actions against COVID-19 correlate with when the WHO declared COVID-19 to be a pandemic?
The WHO plays the role of the central agency responsible for surveillance of infectious diseases, and scholars have long stated that fear is a strong motivator of state action (Alfred 2019, 157). While it would seem that, as the strongest alert the WHO could issue, a PHEIC would trigger a fear response in states, one must also recognize that COVID-19 was not the first time the WHO declared a PHEIC. The designation was given to the swine flu in 2009, polio in 2014, Zika in 2016, and Ebola in 2019 (Caffrey 2024). However, none of these outbreaks rose to the level of COVID-19; none of these diseases was a pandemic. In fact, even the SARS outbreak of 2002-2003, which triggered updates to the IHR, was contained as an epidemic.
Thus, while the notion that COVID-19 is a PHEIC may not have triggered the fears of states, as they could have viewed themselves as equipped to contain it, the WHO’s declaration that COVID-19 is a pandemic did not prompt states to take strong actions given the uncertainty associated with the uncommon label and rapid spread of the disease (Alfred 2019, 157). Interestingly, however, this fear was the reason cited by the WHO Director-General for the WHO’s delay in declaring COVID-19 a pandemic. Even after COVID-19 had spread globally in February 2020 – with cases being found in Asia, North America, Europe, and the Middle East – the WHO decided not to refer to the disease as a pandemic (Harris 2020). The Director-General stated, “a disease needs to have a significant impact on at least two continents for him to consider it a pandemic” and that he “is mindful of the power of a label” (Harris 2020). Despite being armed with the knowledge that the WHO officially defines as a new virus that spreads globally and to which individuals lack immunity, the Director-General stated, “Using the word pandemic does not fit the facts, but it may certainly cause fear. This is not the time to focus on what word we use. That will not prevent a single infection today or save a single life today” (Harris 2020).
The notion that labelling a pandemic may cause fear and yet it may not save lives nor prevent infection is paradoxical; it stands in stark contrast with scholars’ understanding that fear is a key motivator that leads states to take actions against contagions. The Director-General’s statements also demonstrate that the WHO deliberately delayed classifying COVID-19 as a pandemic. While declaring COVID-19 a pandemic on March 11, 2020, the WHO Director-General, Dr. Tedros Adhanom Ghebreyesus, stated that, “We have never before seen a pandemic sparked by a coronavirus, and we have never before seen a pandemic that can be controlled” (Young 2020). The WHO advised that, “If countries detect, test, treat, isolate, trace and mobilize their people in their response, then those with a handful of cases can prevent those cases becoming clusters, and those clusters becoming community transmission” (Young 2020). Therefore, countries after March 11, 2020, were aware that they needed to take immediate action to protect their populations from COVID-19. However, between January 30th and March 11th, seeing as former PHEICs such as Ebola and the Zika virus had not become pandemics, countries were not operating on the possibility that merely since the WHO had declared COVID-19 to be a PHEIC, it required an immediate response, else it would turn into a pandemic.
On that note, since the fear and damage to material interests associated with the severity of a pandemic would motivate states to take actions to protect their populations against COVID-19, the question arises: if the WHO had declared COVID-19 to be a pandemic earlier, would states have addressed COVID-19 more effectively? To respond to this question, this study will now turn to examining Canada’s COVID-19 response and the role played in it by the WHO’s classification of COVID-19 as a PHEIC and pandemic.
Canada’s COVID-19 Interventions Before the WHO’s Pandemic Declaration
Canada’s first case of COVID-19 was confirmed on January 22, 2020. The same week, Canada issued a travel advisory against non-essential travel to China (“Canadian COVID-19 Intervention Timeline” 2022). On January 26, 2020, Foreign Affairs Minister Francois Phillipe-Champagne stated that the travel advisory is “a result of the spread of coronavirus” (“Statement by Foreign Affairs Minister on Travel to Hubei Province in China” 2020). This travel advisory reflects the Canadian government’s view that COVID was contained within China, rather than a globally spread disease. Philippe-Champagne also stated that“Canada does not have a consular presence in Wuhan,” which reveals Canada’s lack of direct access to information on happenings in Wuhan (“Statement by Foreign Affairs Minister on Travel to Hubei Province in China” 2020).
Even after the WHO declared COVID-19 a PHEIC on January 30, 2020, the Canadian government did not take significant action against the virus. In fact, as revealed by CIHI’s Canadian COVID-19 Intervention Timeline, until March 2020, Canada’s interventions were limited to issuing travel advisories for individual countries, besides China, as they began witnessing a large number of COVID-19 cases (2022). However, most of these advisories were issued in late February and early March. To illustrate, the Government of Canada issued the following warnings before the WHO announced COVID is a pandemic on March 11, 2020:
- February 29: advisory against all travel to the affected cities in South Korea.
- March 2: advisory against non-essential travel to affected areas of Italy.
- March 9: advisories against all travel to Iran and all cruise travel.
The actions taken before March 11 align with the notion that the government saw COVID-19 as a controlled outbreak limited predominantly to the regions for which it issued travel advisories. Furthermore, Canada’s increase in advisories on February 29th, 2020, coincided with increasing COVID-19 cases in the country. As of February 22nd, there were 28 documented cases of COVID-19 in Canada; this count rose to 86 by February 29th and 359 by March 7th; before February 22nd, the case count remained below 20 “COVID-19 Epidemiology Update: Current Situation” 2024). Thereby, while the WHO may have declared COVID-19 to be a PHEIC in January, it was not a pressing domestic concern for Canada until March.
The Government of Canada’s understanding that COVID-19 was relatively contained was consistent with the statistics that the WHO released when declaring the virus a PHEIC. The WHO stated there are 7711 confirmed and 12167 suspected cases of COVID-19 in China, while also stating there have only been 82 cases detected outside China (“WHO Declares Public Health Emergency on Novel Coronavirus” 2020). That said, the Pan-American Health Organization’s Assistant Director stated on January 30 that the virus poses a high risk to all countries in the world, in addition to a very high risk to China (“WHO Declares Public Health Emergency on Novel Coronavirus” 2020). However, despite being classified as posing a high risk to all countries, COVID-19 was not classified as a pandemic at the time, nor did statistics seem to indicate a high global spread. Thereby, while the WHO positioned COVID-19 as a concern by calling it high risk and a PHEIC, the virus to common onlookers may not have seemed as if it would rise to the level of a global pandemic.
Canada’s Actions after the WHO Characterized COVID-19 as a Pandemic
On March 11, 2020, the WHO classified COVID-19 as a global pandemic, and Canada’s actions against the pandemic increased dramatically. The WHO’s declaration coincided with the Canadian government encouraging the adoption of work-from-home policies and publishing self-isolation guidelines (“Canadian COVID-19 Intervention Timeline” 2022). Later, on March 26 and 28, Health Canada published guidelines surrounding the optimal use of masks; the department explained the use of masks and respirators for healthcare workers, while also publishing guidelines for non-medical masks to be used among the Canadian populace (“Canadian COVID-19 Intervention Timeline” 2022).
Closing the Border
The travel advisories that had been limited earlier also broadened to all non-essential travel being advised against on March 14 (“Canadian COVID-19 Intervention Timeline” 2022). On March 18, 2020, Canada shut down its borders to foreign nationals departing from all countries besides the United States (Transport Canada 2020). On March 21, 2020, Canada extended this restriction by banning recreational and leisure travel between Canada and the United States (“Canadian COVID-19 Intervention Timeline” 2022). Importantly, Canada implemented exceptions to these restrictions; thereby, the entry of foreign nationals was not completely halted. For instance, air crews and travellers transiting to another country via Canada, Canadian permanent residents, diplomats, and the immediate family of Canadian citizens were allowed to enter the country (Transport Canada 2020).
Transport Canada’s statement concerning “Closing the Borders,” mentioned that as Canada undertakes aggressive efforts to contain the spread of COVID-19, it must also ensure that Canadian “airlines continue to fly, and that supply chains remain open” (2020). This statement highlights that Canada attempted to balance its need to protect Canadians from COVID-19 with safeguarding the economy. Given the significant economic impact that restricting tourism would have, it is understandable why Canada would attempt to delay travel restrictions until it felt it was necessary. In fact, Canada’s effort to minimize disruptions in international travel aligns with the IHR’s central objective of responding to the international spread of disease in a way that “avoids unnecessary interference with international traffic and trade” (Rushton and Ferhani 2021, 3). Canada’s efforts to avoid restrictions that would harm the economy may also be influenced by the fact that the 2008 Financial Crisis had a long-standing impact on the Canadian economy, and pre-crisis monetary policies had only returned in 2017 (Gordon 2017).
Journalists have questioned whether, without this delay in closing borders, Canada could have limited COVID transmission in the country, since, given Canada’s location, most travellers must enter by air (Dyer 2020). While journalists portray the delay as a policy failure, it is also reflective of the fact that COVID-19 was underestimated. As revealed by Daniel Kahneman, many individuals, including medical professionals, did not intuitively recognize that COVID-19 grows exponentially. Given that understanding, when making decisions, both government officials and ordinary citizens focused on the present death rate, not how it would multiply in 2-3 weeks (Corby 2020). Journalists writing about Canada’s border closure months after the fact have the benefit of hindsight; therefore, it is important to zero in on the information available to the government at the time. Given that COVID cases were not increasing rapidly before March 2020, nor had the WHO decreed it as a pandemic. Rather, when decreeing it a PHEIC, the WHO’s statistics positioned COVID-19 as largely affecting China while also posing a risk to the rest of the world. Canada’s response reflects the notion that the exponential growth of COVID-19 was overlooked.
Alternative Solutions – Was Closing the Border Necessary?
That said, closing the borders was not the only option available to Canada. In fact, by March 2020, when Canada closed its borders to foreign nationals, COVID-19 was already present in the country, and the number of cases was multiplying. Between March 14 and April 18, cases multiplied from 1,590 to 10,407 (“COVID-19 Epidemiology Update: Current Situation” 2024). While this number could have been higher without border closures, the continued rapid spread despite border closures underscores that other factors beyond lack of travel restrictions influenced Canada’s failure to contain COVID-19.
Failing to Recognize COVID’s Airborne Transmission
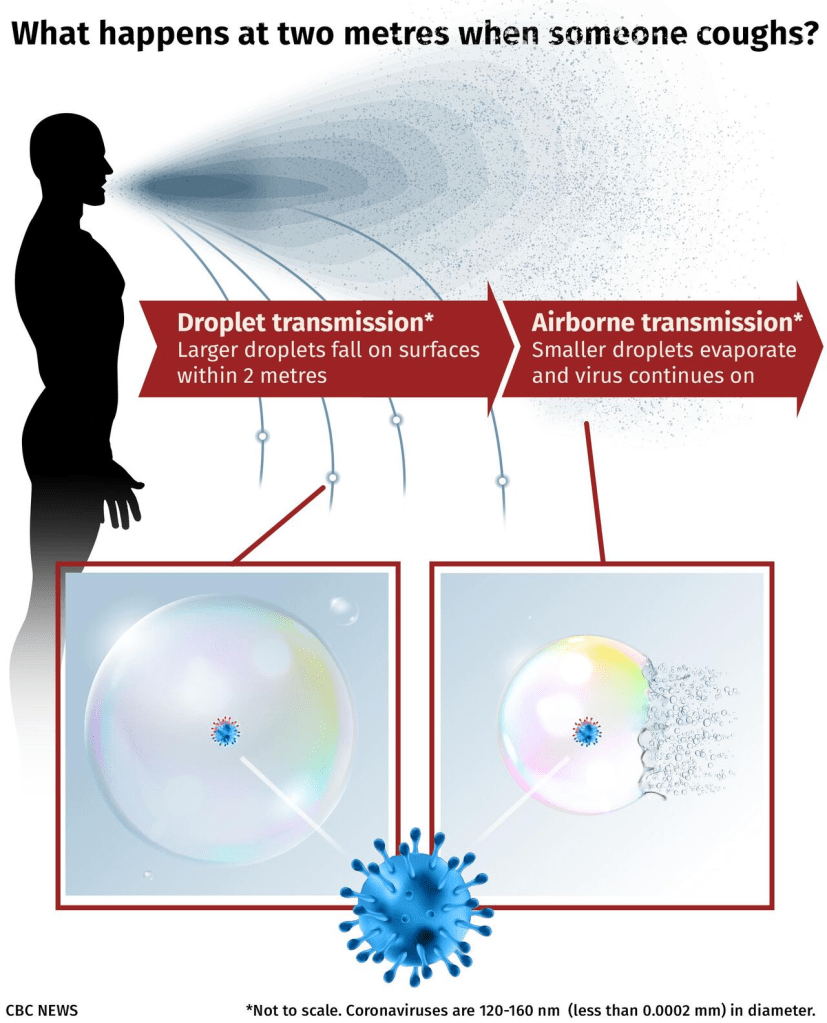
Figure 1: CBC Illustration Demonstrating Airborne Transmission
A key failure in Canada’s response was inaccurate guidelines. The Public Health Agency of Canada (PHAC), until November 2020, stated that COVID-19 spreads through “breathing in respiratory droplets, touching contaminated surfaces and common greetings like handshakes and hugs” (Miller 2020). In November, this guidance was updated to include that the virus spreads through aerosols, i.e. microscopic airborne particles, created “when an infected person coughs, sneezes, sings, shouts, or talks” (Miller 2020). Pre-November guidelines yielded emphasis on social distancing as a prevention measure; however, the prescribed 2 metre distance only protects against droplet transmission, not airborne transmission. Insightful graphics were shared by CBC News explaining this phenomenon to Canadians (See Figure 1; Miller 2020).
The failure of Canadian health officials to recognize this transmission method sooner led to Canadians being at risk and contracting COVID-19 despite following what they were told were the necessary steps to prevent COVID-19 infections. Furthermore, as explained by Michael Brauer, a Professor at the UBC School of Population and Public Health, COVID-19 being airborne entailed that disinfecting surfaces was not an effective prevention measure, as it is “extremely rare for the virus to spread through surface contact,” and rather constant disinfection in itself could be damaging to individuals’ health (CBC Radio 2021). He instead emphasized the need for ventilation, distancing more than two metres, doing activities outdoors rather than indoors wherever possible; the pre-existing strategy Brauer affirmed was masking (CBC Radio 2021).
Having identified that the failed recognition of COVID-19’s transmission method was a pivotal shortcoming in Canada’s pandemic response, this study now turns to examining whether this was a preventable failure, by exploring whether it was possible for Canada to have known earlier that COVID-19’s primary route of transmission is airborne transmission. Given that other states recognized this transmission method early in the pandemic, Canada had access to knowledge through which it could have easily determined that COVID-19 was airborne. Thereby, it could have adjusted its prevention strategies accordingly. To illustrate, a model created by Aalto University in Finland in April 2020, which was shared publicly, also supported airborne transmission of microdroplets (Reals 2020). Similarly, Japan recognized the virus as airborne months before the WHO decreed it as such in July 2020 (Craft 2020). Moreover, despite the WHO having confirmed COVID-19’s airborne transmission in July, Canada did not update its public health guidelines until November 2020. Therefore, Canada failed to act on knowledge that would have allowed it to issue accurate public health guidelines, significantly prevent transmission between April and November 2020, and thereby contain the spread of COVID-19 in the country.
March Break: Communication Gaps between Federal and Provincial Governments
In Canada, the responsibility for healthcare is shared by the federal and provincial governments. While provincial governments are responsible for administering healthcare, they do so in accordance with funding and national standards that are decided by the federal government (“What Role Does the Federal Government Play in Health Care?” 2025). The Canada Health Act governs the country’s publicly funded healthcare system, which “provides coverage for primary health care services, from diagnosis to recovery” (Government of Canada 2025).
This division of jurisdiction over healthcare translated to inconsistent healthcare policies across Canada’s provinces. Importantly, March 16th to March 20th was March Break, where students had a week of break from school. While the Ontario government ultimately extended the break due to COVID-19, it did not advise any caution before the break (“Toronto District School Board Calendar” 2020; Rushowy and Benzie 2020). Rather, Ontario Premier Doug Ford stated families “were safe to travel” during March Break, because he had not received any federal guidelines implying otherwise. On March 16th, the first day of March Break, Prime Minister Justin Trudeau announced Canada was shutting its borders to foreign nationals. Contrary to Ford’s declaration that travel was safe, Trudeau, when addressing Canadian nationals abroad, stated, “It is time for you to come home” (Vahed 2021). Meanwhile, British Columbia’s provincial government had already cautioned against non-essential travel during March Break (Vahed 2021). These differing policies highlight the lack of communication between provinces and the federal government.
Additionally, while the federal government closed borders, there were no measures put in place to prevent transmission from the returning March Break travellers. An Emergency Order was implemented on March 25, which subjected travellers to a mandatory quarantine (Vahed 2021). However, given that Trudeau called Canadians home on March 16th, and March Break ended on March 20th, this Emergency Order did not prevent transmission from March Breakers who had contracted COVID-19 on their trips. That said, the Ontario Government’s extended closure of schools post-break may have prevented some transmission in Ontario. Despite any potential success due to the actions of Ontario and British Columbia’s provincial governments, the lack of coordinated federal-provincial policy fueled Canada’s failure to contain COVID-19.
Failure to Maximize the Global Public Health Intelligence Network (GPHIN)
Finally, perhaps the greatest shortfall in Canada’s COVID-19 response was that it failed to respond to the virus despite being home to the intelligence technology that detected it on December 30th in Wuhan. Headquartered in Ottawa, the Global Public Health Intelligence Network (GPHIN) is a collaborative effort between the WHO and Canada; it has been responsible for tracking biological threats across the globe since 1997 (Fitzgibbon 2021, 4; Levy 2021, 3; “About GPHIN” 2025). GPHIN “identified the outbreak of pneumonia of unknown cause in Wuhan, China, that would become COVID-19 on December 30, 2019, noted it on a Daily Report on December 31, 2019, and issued a special report on January 1, 2020” (Levy 2021). Adrian Levy (2021) accurately characterized GPHIN as “the crown jewel in Canada’s biological surveillance apparatus,” as GPHIN captured around 7,000 global news items daily. Nonetheless, GPHIN’s findings did not impact decision-making; this lack of impact occurred because before COVID-19, the Canadian government had “siloed” its greatest tool (Levy and Wark 2021).
As affirmed by a May 2021 independent review panel, Canada did not fully leverage GPHIN’s intelligence due to structural problems within PHAC (Levy 2021, 3). Thereby, despite GPHIN issuing daily reports on the detected virus after January 1, Canada remained under the illusion that it was prepared to address COVID-19 effectively (Levy 2021, 3). GPHIN’s daily reports were circulated within PHAC and to the provinces and territories, but they contained lengthy media summaries, which weakened their utility in decision-making (Fitzgibbon 2021, 4). Neither the provincial nor the federal government maximized the intelligence found by GPHIN, and thereby they failed to protect Canada from the catastrophes unleashed by COVID-19.
Conclusion
Turning to the recent past, SARS-CoV-1 was also a coronavirus, yet it was contained between 2002-2003. When commenting on SARS, Thomas Tsang stated that if the appropriate control measures had not been taken, the outbreak could have been a global pandemic (Price-Smith 2008, 142). Tsang’s foreshadowing came to life when SARS-CoV-2, i.e. COVID-19, emerged and became a global pandemic. Despite public health having risen to the level of “high politics” in Ottawa, the Canadian government failed to contain COVID-19 when it reached the country in 2020 (Price-Smith 2008, 147).
Canada’s response to COVID-19 encompassed shortcomings that were independent of the WHO’s pandemic declaration. There was a lack of communication between the federal and provincial governments surrounding travel during March Break, and measures to quarantine afterwards. Despite March Break beginning on the 16th, and the WHO having declared COVID-19 to be a pandemic on the 11th, the Trudeau government did not take action to advise the provinces, nor Canadian citizens, against travel. The provinces were not made aware of the upcoming travel ban until Trudeau announced it on March 16th, at which point, many Canadians had departed the country and would return with COVID-19.
The WHO also contributed to Canada’s failure to contain COVID-19 through its delay in classifying the coronavirus as a PHEIC, and more importantly, by delaying naming it a pandemic. While pandemic is not a formal classification that the WHO is responsible for declaring, the WHO’s role as the central agency responsible for surveilling infectious diseases confers it with authority and credibility that leads to states taking actions based on its announcements. Since PHEIC is a designation that has been given to diseases which did not rise to the level of a pandemic, titling COVID-19 accurately as a pathogen that had spread globally was vital to triggering states’ responses. The WHO’s ability to influence global health policies across the globe is a key manifestation of the understanding that International Organizations are active participants in international relations who have authority and autonomy.
States take actions against contagions due to fear and an attendant threat to their material interests (Price-Smith 2008, 157). COVID-19, being a pandemic, satisfied both these factors. The notion of COVID-19 rising to an unprecedented level, with perhaps the closest precedent being the Spanish Flu of 1918, produced fear and uncertainty. Further, the severity of the pandemic also meant it would have significant impacts on states’ material interests. The WHO’s Director-General acknowledged the significant impact that would ensue as a result of the WHO labelling COVID-19 a pandemic; however, he failed to understand that the fear and impact would motivate states to take rapid action to protect their populations and interests from the coronavirus. Contrary to his claim, an earlier declaration of a pandemic from the WHO once the virus had evidently spread globally could have saved lives and prevented infections.
If Canada had maintained its flawed response but acted faster due to an earlier WHO pandemic declaration, it would have been able to reduce the number of COVID-19 cases. This acceleration would not have resolved the shortcomings in Canada’s healthcare system nor prevented the airborne transmission that ensued due to inaccurate guidelines, but it could have prevented the transmission that occurred due to March Break travel. That said, had Canada effectively communicated between its provinces and addressed the flaws in its healthcare system, it could have counteracted the WHO’s delayed characterization. Moreover, since GPHIN was responsible for detecting the novel coronavirus and that it is the most advanced technology available to detect biological threats, had Canada maximized the intelligence it gained from GPHIN, it may have counteracted the detrimental impact from the WHO’s delayed characterizations of COVID-19.
On balance, the WHO’s delayed declaration of a pandemic influenced Canada’s failure to effectively contain COVID-19 to some extent, but domestic shortcomings were equally, if not more, responsible for Canada’s failed response to COVID-19. Thereby, Canada’s response to COVID-19 demonstrates a combined domestic and international failure to prevent the catastrophic spread of an infectious disease.
References
1. Alfred, Natalie. 2019. “How Fear Shapes World Politics.” E-International Relations. May 6, 2019. https://www.e-ir.info/2019/05/06/how-fear-shapes-world-politics/.
2. Barnett, Michael. 2020. “COVID-19 and the Sacrificial International Order.” International Organization 74 (S1): E128–47. https://doi.org/10.1017/S002081832000034X.
3. Caffrey, Cait. 2024. “Public Health Emergency of International Concern.” EBSCO. 2024. https://www.ebsco.com/research-starters/health-and-medicine/public-health-emergency-international-concern.
4. “Canada’s Internet Factbook 2019.” 2019. CIRA. Canadian Internet Registration Authority. April 2019. https://www.cira.ca/en/resources/documents/about/canadas-internet-factbook-2019/.
5. “Canadian COVID-19 Hazard Index.” 2025. COVID-19 Resources Canada. 2025. https://covid19resources.ca/covid-hazard-index/.
6. “Canadian COVID-19 Intervention Timeline.” 2022. Canadian Institute for Health Information. October 13, 2022. https://www.cihi.ca/en/canadian-covid-19-intervention-timeline.
7. CBC Radio. 2021. “Coronavirus Is Airborne so Stop Disinfecting Everything: Expert.” CBC. May 14, 2021. https://www.cbc.ca/radio/whitecoat/coronavirus-is-airborne-so-stop-disinfecting-everything-expert-1.6022520.
8. Corby, Rhiannon. 2020. “Why We Underestimated COVID-19.” The New Yorker Radio Hour. WNYC Studios. 2020. https://www.wnycstudios.org/podcasts/tnyradiohour/segments/why-we-underestimated-covid-19.
9. “COVID-19 Epidemiology Update: Current Situation.” 2024. Government of Canada. October 1, 2024. https://health-infobase.canada.ca/covid-19/current-situation.html.
10. Craft, Lucy. 2020. “Japan Has Long Accepted COVID’s Airborne Spread, and Scientists Say Ventilation Is Key.” CBS News. July 13, 2020. https://www.cbsnews.com/news/coronavirus-japan-has-long-accepted-covids-airborne-spread-and-scientists-say-ventilation-is-key/.
11. Dyer, Evan. 2020. “COVID-19 Taught Canada a Costly Lesson — That Early Border Closures Can Work.” CBC, June 23, 2020. https://www.cbc.ca/news/politics/covid-coronavirus-pandemic-trudeau-borders-1.5619705.
12. Fitzgibbon, Joy. 2021. “WHO, Infectious Disease Surveillance and COVID-19.” Canadian International Council: Behind the Headlines 69 (7): 1–4. https://thecic.org/wp-content/uploads/2021/02/Joy-Fitzgibbon-1.pdf.
13. Geddes, Linda. 2023. “COVID-19 Is No Longer a Public Health Emergency of International Concern. Does This Mean the Pandemic Is Over?” Vaccines Work. Gavi: The Vaccine Alliance. May 5, 2023. https://www.gavi.org/vaccineswork/covid-19-no-longer-public-health-emergency-international-concern-does-mean-pandemic.
14. Gordon, Stephen. 2017. “Recession of 2008–09 in Canada.” The Canadian Encyclopedia. Historica Canada. October 24, 2017. https://thecanadianencyclopedia.ca/en/article/recession-of-200809-in-canada.
15. Government of Canada. 2025. “About Canada’s Health Care System.” Government of Canada. June 25, 2025. https://www.canada.ca/en/health-canada/services/canada-health-care-system.html.
16. Harris, Richard. 2020. “Why Is the WHO Not Calling the Coronavirus a Pandemic?” NPR. February 25, 2020. https://www.npr.org/2020/02/25/809182758/why-is-the-who-not-calling-the-coronavirus-a-pandemic.
17. “Health Topics: Pandemics.” 2025. World Health Organization. 2025. https://www.who.int/health-topics/pandemics.
18. Levy, Adrian R. 2021. “After COVID: Global Pandemics and Canada’s Biosecurity Strategy.” Centre for International Governance Innovation. https://www.cigionline.org/publications/after-covid-global-pandemics-and-canadas-biosecurity-strategy/.
19. Levy, Adrian R., and Wesley Wark. 2021. “The Pandemic Caught Canada Unawares: It Was an Intelligence Failure.” Centre for International Governance Innovation. Autumn 7, 2021. https://www.cigionline.org/articles/the-pandemic-caught-canada-unawares-it-was-an-intelligence-failure/.
20. Miller, Adam. 2020. “Canada Quietly Updates COVID-19 Guidelines on Risk of Airborne Spread.” CBC, November 4, 2020. https://www.cbc.ca/news/health/coronavirus-canada-aerosol-transmission-covid-19-1.5789906.
21. “Pandemic Prevention, Preparedness and Response Accord.” 2025. World Health Organization. June 27, 2025. https://www.who.int/news-room/questions-and-answers/item/pandemic-prevention–preparedness-and-response-accord.
22. Price-Smith, Andrew T. 2008. “Epidemic of Fear: SARS and the Political Economy of Contagion in the Pacific Rim .” In Contagion and Chaos, 139–57. MIT Press.
23. “Public Health Agency of Canada’s COVID-19 Response: Lessons Learned.” 2024. Government of Canada. June 13, 2024. https://www.canada.ca/en/public-health/corporate/transparency/corporate-management-reporting/evaluation/covid-19-response-lessons-learned-summary.html.
24. Reals, Tucker. 2020. “This Is How Coughing Can Spread Coronavirus in a Grocery Store, according to Researchers.” CBS News. April 9, 2020. https://www.cbsnews.com/news/coronavirus-coughing-spread-covid-19-grocery-store-researchers/.
25. Rushowy, Kristin, and Robert Benzie. 2020. “Ontario Schools to Shut down for Two Weeks after March Break to Fight the Spread of COVID-19.” Toronto Star. March 12, 2020. https://www.thestar.com/politics/provincial/ontario-schools-to-shut-down-for-two-weeks-after-march-break-to-fight-the-spread/article_4e09feee-399b-5b73-b751-25203c449126.html.
26. Rushton, Simon, and Adam Ferhani. 2021. “The International Health Regulations, COVID-19 and National Borders: Pursuing Health Security in a Globalized World.” Canadian International Council: Behind the Headlines 69 (6): 1–4. https://thecic.org/wp-content/uploads/2021/02/Rushton-and-Ferhani-Final-1.pdf.
27. Stasavage, David. 2020. “Democracy, Autocracy, and Emergency Threats: Lessons for COVID-19 from the Last Thousand Years.” International Organization 74 (S1): E1–17. https://doi.org/10.1017/S0020818320000338.
28. “Statement by Foreign Affairs Minister on Travel to Hubei Province in China.” 2020. Government of Canada. January 26, 2020. https://www.canada.ca/en/global-affairs/news/2020/01/statement-by-foreign-affairs-minister-on-travel-to-hubei-province-in-china.html.
29. “The Daily: Household Internet Use Survey.” 2003. Statistics Canada. Government of Canada. September 18, 2003. https://www150.statcan.gc.ca/n1/daily-quotidien/030918/dq030918b-eng.htm.
30. “Toronto District School Board Calendar.” 2020. 2020. https://schoolweb.tdsb.on.ca/Portals/tomlongboat/docs/Calendar%202019-2020.pdf.
31. Transport Canada. 2020. “Closing the Borders.” Public Safety Canada. 2020. https://www.publicsafety.gc.ca/cnt/trnsprnc/brfng-mtrls/prlmntry-bndrs/20200724/041/index-en.aspx.
32. United Nations. n.d. “14.9 Million Excess Deaths Associated with the COVID-19 Pandemic in 2020 and 2021.” United Nations. Accessed November 30, 2025. https://www.un.org/en/desa/149-million-excess-deaths-associated-covid-19-pandemic-2020-and-2021.
33. Vahed, Marium Nur. 2021. “COVID-19 Federalism: Disparate Government Responses in Canada.” Munk School of Global Affairs & Public Policy. January 4, 2021. https://munkschool.utoronto.ca/research/covid-19-federalism-disparate-government-responses-canada.
34. Waal, Alex de. 2020. “New Pathogen, Old Politics.” Boston Review. April 3, 2020. https://www.bostonreview.net/articles/alex-de-waal-thining-critically-pandemic/.
35. “What Role Does the Federal Government Play in Health Care?” 2025. Canadian Medical Association. March 25, 2025. https://www.cma.ca/latest-stories/what-role-does-federal-government-play-health-care.
36. “WHO Declares Public Health Emergency on Novel Coronavirus.” 2020. Pan American Health Organization. World Health Organization. January 30, 2020. https://www.paho.org/en/news/30-1-2020-who-declares-public-health-emergency-novel-coronavirus.
37. World Health Organization. 2019. “Emergencies: International Health Regulations and Emergency Committees.” World Health Organization. December 19, 2019. https://www.who.int/news-room/questions-and-answers/item/emergencies-international-health-regulations-and-emergency-committees.
38. World Health Organization. 2025. “Coronavirus Disease (COVID-19) Pandemic.” World Health Organization. 2025. https://www.who.int/europe/emergencies/situations/covid-19.
39. World Health Organization. 2025. “WHO Scientific Advisory Group Issues Report on Origins of COVID-19,” June 27, 2025. https://www.who.int/news/item/27-06-2025-who-scientific-advisory-group-issues-report-on-origins-of-covid-19.
40. Young, Leslie. 2020. “WHO Declares Novel Coronavirus Disease a Pandemic.” Global News. March 11, 2020. https://globalnews.ca/news/6660863/who-coronavirus-pandemic.
